
Marijuana has gone mainstream. The plant, its sister hemp, and their constituents now show up in oils, creams, candies, and more. Putting aside the many controversies over marijuana, here’s what it does for—or to—your health.
“Ten years ago, when you referred to cannabis, you were talking about dried plant material that people smoked,” says Ryan Vandrey, associate professor of psychiatry and behavioral sciences at the Johns Hopkins School of Medicine.
“Now, cannabis—which refers to marijuana and hemp—is a blanket term that could also mean hemp oil, topical creams, CBD products, high-THC concentrates that are smoked, vaporized, or orally ingested, and more.”
And confusion abounds. “People either demonize cannabis or make it sound like the most amazing thing,” says Vandrey.
The truth likely falls somewhere in the middle.
“Maybe cannabis will be useful to some people, but it will be disappointing to most,” says Daniele Piomelli, professor of anatomy and neurobiology at the University of California, Irvine.
“Cannabis will not be a panacea. Nor will it be as dangerous as some people think.”
Here are 10 things you should know about cannabis.
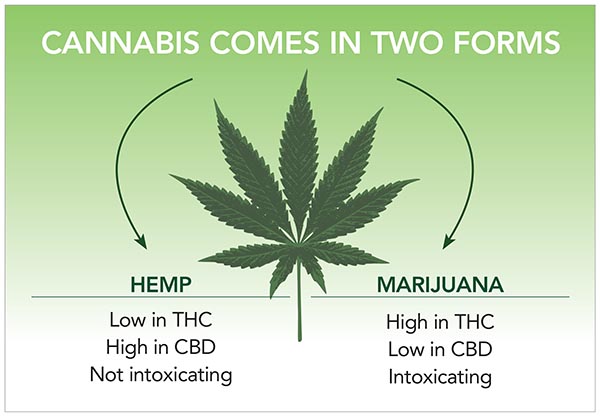
1. Don’t confuse THC with CBD.
Cannabis plants contain a class of compounds called cannabinoids.
“We’ve identified just over 100 of them,” says Piomelli. The two most abundant: tetrahydrocannabinol (THC) and cannabidiol (CBD).
“THC drives the hallmark features of feeling high, like getting the munchies and feeling relaxed, as well as the negative side effects, like feeling paranoid or anxious,” explains Vandrey.
(In recent years, marijuana’s potency has soared. In 1980, marijuana averaged about 1 percent THC.1 In a recent report, marijuana sold at dispensaries averaged 21 percent THC, according to labels.2)
“CBD can produce drug effects, but it’s not the typical marijuana high,” notes Vandrey. “It’s not intoxicating, and it doesn’t come with THC-like side effects.”
Hemp oil doesn’t have much CBD unless it’s added, because CBD is found only in hemp’s leaves and flowers (not its seeds). So if you want CBD, look for CBD—not cannabinoids—on the label.
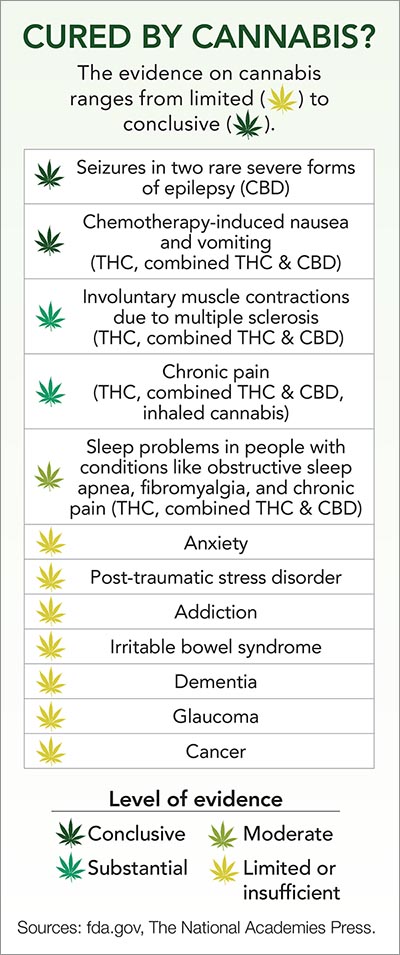
2. Cannabis has few established medical benefits.
In 2017, a National Academy of Medicine panel drew roughly 100 conclusions on the health effects of cannabis (see “Cured by Cannabis?” below).3 Only three benefits stood out:
■ “We found conclusive evidence that cannabis can reduce nausea and vomiting induced by chemotherapy,” says Piomelli, who served on the panel.
■ There is “substantial” evidence that cannabis modestly reduces self-reported involuntary muscle contractions in people with multiple sclerosis.
■ There is “substantial” evidence that cannabis modestly reduces chronic pain. “It’s not as strong as a narcotic pain reliever like an opiate,” Piomelli notes. “So it’s not as effective, but it may be more usable long term.”
As for most other health problems, few good studies have been done. But the list of cannabis’s benefits may never be long.
“In what other case do we have a single medicine that we use to treat 30 different health conditions?” says Vandrey.
In fact, the Food and Drug Administration has approved just three (synthetic) THC drugs—Marinol and Syndros (dronabinol) and Cesamet (nabilone)—to treat nausea and vomiting from chemotherapy. (That’s how cannabis should be tested and sold as medicine.)
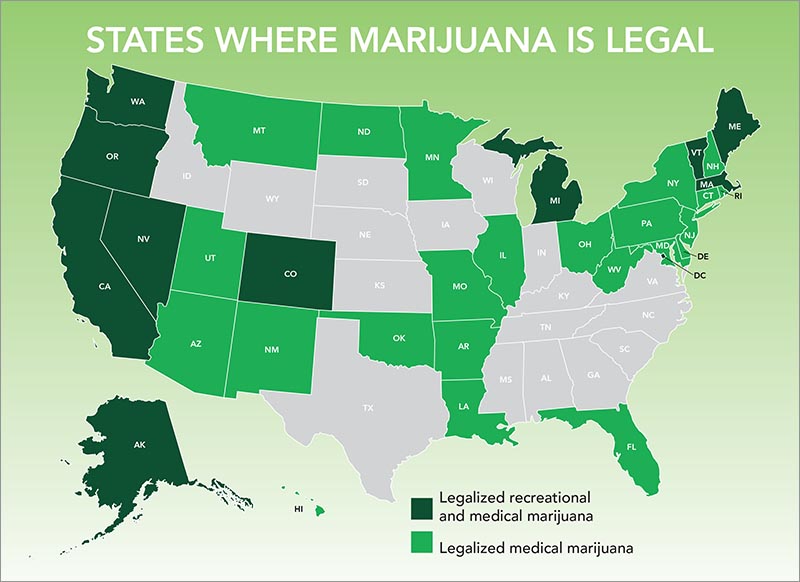
But some states are far more enthusiastic. “In many, the list of conditions for which medical cannabis is authorized is very long,” says Piomelli.
“Out of those, we really have evidence for maybe one or two.”
3. The evidence for CBD is scant.
You can buy CBD as an oil, but it’s also sold in everything from water and candy to Willie Nelson’s CBD-infused coffee.
“CBD is promoted as this amazing, natural, healing product,” says Vandrey. “But many claims about CBD haven’t been substantiated in humans.”
Not that CBD is worthless. Last year, the FDA approved a high-dose CBD drug to treat seizures in two rare severe forms of epilepsy.4 But beyond that, the evidence is preliminary.
Only a few studies have looked at whether CBD relieves anxiety, the most common claim.
In one trial, 57 Brazilian men were randomly assigned to take a placebo or 150, 300, or 600 milligrams of CBD 90 minutes before giving a speech. Oddly, only those who took 300 mg reported lower anxiety during—but not before or after—the speech than placebo takers.5 (Most of the study’s authors had ties to the CBD industry.)
No long-term trials have tested CBD for occasional anxiety or to treat people with a diagnosed anxiety disorder.
And most studies have used doses of 100 mg or more. Few CBD products have more than 20 mg per dose.
“People are throwing CBD at every condition under the sun at random doses and expecting it to work,” says Vandrey.
“There are a lot of possibilities for CBD,” notes Piomelli, “but they require controlled clinical trials. The smoking gun isn’t there yet.”
4. CBD can interfere with medicines.
In animal and test-tube studies, CBD blocks some forms of an enzyme—cytochrome P450—that metabolizes many medicines, including some statins, calcium channel blockers, and antidepressants.6
“We know that CBD can affect the metabolism of drugs, though the extent to which that happens is still not well understood,” says Vandrey.
If you’re considering taking CBD, ask your doctor or pharmacist if it could interfere with your medications.
5. Smoking marijuana can harm your lungs.
“Smoking is probably the worst possible way of getting marijuana into your body,” notes Piomelli.
That’s because smoking marijuana produces many of the same harmful chemicals and carcinogens as smoking tobacco. Yet marijuana smokers don’t have a higher risk of lung cancer than non-smokers.3
“That was one of the biggest surprises of the National Academy of Medicine report,” says Piomelli.
The dose may explain why. “Tobacco smokers might smoke 20 or 40 cigarettes a day,” notes Piomelli. “I’ve never heard of someone smoking 40 joints a day.”
But smoking marijuana does increase the risk of chronic bronchitis and worsens respiratory symptoms like coughing and wheezing, said the Academy.3
Some small studies suggest that “vaping”—when marijuana is heated, not burned, and its vapors inhaled—may cause fewer respiratory symptoms.7 But no long-term studies have looked.
6. Cannabis ups your risk of a car crash.
“We know from good, controlled research studies that cannabis impairs driving,” says Vandrey.8 But if a driver is in a crash and tests positive for THC, “we have no good way to know whether that person was intoxicated or under the influence at the time of the accident.”
That’s because THC can be detected in blood long after the user is no longer impaired.
What’s more, blood levels of THC increase rapidly after you’ve inhaled marijuana, but they stay low—below the limit that many state tests can detect—after you’ve had an edible (a food or drink that contains THC).
“Unlike alcohol, blood levels of THC do not reflect intoxication,” says Piomelli.
7. Cannabis has other risks.
“Cannabis has the same types of effects on the reward pathway in the brain as alcohol, cocaine, opioids, and nicotine,” says Vandrey.
But the risk of cannabis abuse is fairly low. “Most people who use cannabis won’t have issues with it,” Vandrey notes. “The current estimate is that about 10 percent of people who try it will end up having problems.”
That’s concerning, but it’s less than the roughly 20 percent of drinkers or 65 percent of nicotine users who become dependent.9
The Academy also found “substantial” evidence that cannabis use may increase the risk of psychotic disorders like schizophrenia, with the highest risk among the most frequent users.
“Young adolescents also have a higher risk,” says Vandrey. “But a cause-and-effect relationship hasn’t been established for any group.” Still, he adds, “people with a family history of psychosis should avoid cannabis, especially products with high THC content.”
8. Don’t trust labels.
“You can’t rely on labels,” says Piomelli. In states that test cannabis products, the results are troubling.
For example, in 2018 the California Bureau of Cannabis Control tested nearly 26,000 products—plant material, vape pen cartridges, waxes, oils, tinctures, topical creams, edibles—sold at dispensaries. Almost 15 percent failed tests for potency or purity, typically because they were mislabeled or had detectable levels of pesticides, microbes, or solvents.
CBD-only products sold online or in stores fare no better. For example, only about 30 percent of 84 CBD products that Vandrey bought online were accurately labeled.10
“Some contained little to no CBD,” he says. And roughly one in five had detectable levels of THC. “It’s quite possible that the therapeutic benefits people are reporting from CBD are driven by THC, or maybe something else entirely.”
9. A dose of THC varies.
It’s up to each state to decide on an appropriate dose. In Washington and Colorado, for example, a dose of THC is 10 milligrams. In Oregon, it’s 5 mg.
“There’s a fairly narrow dose window between somebody being okay and someone having uncomfortable adverse effects with THC,” Vandrey explains.
He randomly assigned 17 infrequent marijuana users to smoke or vape marijuana with either 0, 10, or 25 mg of THC. Two people vomited and one hallucinated after taking 25 mg, but not 10 mg.11
And when people inhaled 25 mg—but not 10 mg—of THC, they reported feeling more uncomfortable, sick, or anxious than when they inhaled the marijuana with no THC.
What’s more, people were more intoxicated after vaping than after smoking the marijuana.
The take-home message: If you try THC, start low. That means around 2 to 3 mg. “Work your way up slowly until you get the effect you want,” says Piomelli.
“And treat it with respect. This is not a toy. This is a drug. I’m concerned that people think, ‘Oh, it’s natural. It can’t harm me.’”
10. Edibles: the Wild West.
“THC edibles are problematic,” says Piomelli. “It’s easy to eat a cookie without knowing what’s in it.”
And many edibles have much more than 5 to 10 mg of THC.
For example, Dixie Elixirs’ line of 8.5 oz. juices has 100 mg of THC per bottle, but the labels list a serving as 6 mg of THC. Only people who use the “dosing cap” will get the three-teaspoon serving of juice that contains 6 mg of THC.
And keep your edibles away from children. The Poison Control Center warns that some kids have gotten into their parents’ supplies.
Another potential problem: “When you inhale cannabis, you feel the effects almost immediately,” says Vandrey. But it can take 30 to 90 minutes to feel the effects of an edible. If you don’t know that, you may think the dose is too low. “So then you eat more and you’re stoned for hours and hours,” says Piomelli.
What’s more, the kind of food may affect how quickly the THC is absorbed.
“Let’s say you have a lollipop, a gummy bear, and a brownie, each with 10 mg of THC,” says Vandrey.
“When you suck on the lollipop, you absorb some of the THC through the oral mucosa that lines your mouth. That absorption might be much faster than if you eat the gummy bear or the brownie. And if you eat the brownie, the absorption may be much slower if it has a lot of fat.”
“That begs the question: Why does it have to be in a lollipop, gummy bear, or brownie when it should be in a capsule?”
The answer is more about marketing than medicine.
1J. Forensic Sci. 45: 24, 2000.
2J. Gen. Intern. Med. 33: 1426, 2018.
3The National Academies Press 2017. doi:10.17226/24625.
4 fda.gov/newsevents/newsroom/pressannouncements/ucm611046.htm.
5Braz. J. Psychiatr. 2018. doi:10.1590/1516-4446-2017-0015.
6Cannabis Cannabinoid Res. 2: 139, 2017.
7Int. J. Drug Policy 52: 87, 2018.
8Clin. Chem. 59: 478, 2013.
9Drug Alcohol Depend. 115: 120, 2011.
10JAMA 318: 1708, 2017.
11JAMA Netw. Open 1: e184841, 2018.
Photo: Esteban Lopez/unsplash.com (top).