Celiac disease is on the rise. Is it because of how we grow wheat? Can you be sensitive to gluten—a protein found in wheat, barley, and rye—without having celiac? Should you buy an at-home antibody kit to test yourself? Can you trust gluten-free packaged and restaurant foods? Here’s what you need to know.
Benjamin Lebwohl is a gastroenterologist and the director of clinical research at the Celiac Disease Center at Columbia University. His research focuses on the causes and long-term outcomes of celiac disease as well as strategies to improve patients’ quality of life. Lebwohl spoke with Nutrition Action’s Caitlin Dow.
Celiac basics
Q: Why do people with celiac disease react to gluten?
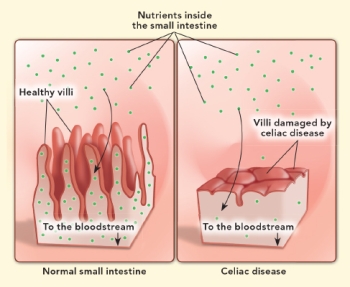
A: Celiac disease is an autoimmune condition where immune cells in the small intestine mistake gluten for a threat. The immune system sees gluten like it’s a pathogen, similar to a bacteria or virus.
In response, the immune cells make antibodies and inflammatory proteins to deal with the perceived threat. That results in collateral damage to the villi of the intestine, which are the long finger-like projections that increase nutrient absorption by maximizing the surface area of the intestine’s lining.
Q: What’s the consequence of that damage?
A: It reduces the intestine’s ability to absorb nutrients, which affects other body systems. For example, bone health takes a hit due to malabsorption of calcium and vitamin D. Anemia is also an issue due to impaired absorption of iron, folic acid, and vitamin B-12.
Q: How common is celiac disease?
A: Somewhere around 0.7 to 1 percent of the population has it. That includes people with undiagnosed celiac disease, which may be about half of people with celiac disease.
Q: Is celiac disease inherited?
A: Yes. There are two genetic markers. Without at least one of them, it’s close to impossible to develop celiac disease.
But they’re very common. Around 30 to 40 percent of us have at least one of them, though about 97 percent of those people never develop celiac. But if you have a first-degree relative—that is, a parent, child, or sibling—with celiac disease, your risk of having celiac rises from roughly 1 percent to 10 percent.
Q: Why do only some people with the gene get celiac?
A: There seems to be some environmental trigger—perhaps an intestinal infection—that leads some people to develop celiac.
There’s more celiac disease now than there was a generation ago. That suggests that there are important environmental determinants because our genetics haven’t changed over a generation, though increased awareness and improved diagnostic techniques may have played a role.
Q: Determinants like what?
A: The most widely accepted theory is related to the hygiene hypothesis. We have less exposure to germs, fewer early-life infections, and greater use of antibiotics, which means that the immune system hasn’t gotten enough practice learning what’s a real threat. Those changes in hygiene may have contributed to the rise of certain autoimmune conditions, including celiac disease.
Q: Are we also eating more wheat?
A: In fact, we eat less wheat now than we did at the turn of the 20th century. There’s also a lot of online misinformation about genetically modified wheat. There is no GMO wheat in the food supply. And it’s likely that the gluten content of wheat hasn’t changed drastically over time.
Diagnosing celiac
Q: What are the signs and symptoms of celiac disease?
A: It is a real chameleon when it comes to symptoms. Some people have many and some have zero. Most, however, fall somewhere in between.
Some of the most common symptoms include weight loss, diarrhea, abdominal pain, and bloating, though constipation can also sometimes be a symptom. Some people have anemia, elevated liver enzymes, peripheral nerve damage, headache, female infertility, or balance issues. And in children, falling off the growth curve can be a sign.
Q: How do people with no symptoms get diagnosed?
A: From screening due to their family history or because they have type 1 diabetes, which is also an autoimmune disorder. People with type 1 diabetes have about an eight-fold increased risk of celiac disease. It’s a well-established link, though not completely understood. People with one autoimmune condition often have others.
Q: Is celiac often missed by doctors?
A: Yes. Many people with celiac disease may have been told many years prior that they have some other condition like irritable bowel syndrome, because the symptoms can overlap.
Q: How is celiac diagnosed?
A: The first step is a blood test. The most reliable marker is an antibody called tissue transglutaminase—or tTG-IgA.
If the antibody is abnormally elevated, the next step is a biopsy of the duodenum, the first part of the small intestine. If the biopsy shows damage to villi, then you get a diagnosis of celiac disease.
Q: Are at-home celiac tests reliable?
A: Even if an at-home test shows elevated antibodies, you still need an intestinal biopsy to confirm the diagnosis. These tests could lead people to bypass a formal diagnosis and adopt a gluten-free diet when it’s not necessary.
Q: Who should get tested for celiac?
A: Certainly anyone with irregular bowel habits or a diagnosis of irritable bowel syndrome. Unexplained weight loss, iron-deficiency anemia, osteoporosis, or female infertility can also be cause for testing.
And possibly people with no symptoms who are at increased risk because they have type 1 diabetes or first-degree relatives with celiac disease.
Q: What’s the harm in not testing?
A: For people with symptoms, the downside is that you’ll have untreated symptoms that impair your quality of life.
And untreated celiac and ongoing intestinal damage may increase the risk of long-term consequences like cancer. For example, people with celiac have a four-fold increased risk of non-Hodgkin lymphoma. It’s likely that with diagnosis and treatment, that risk goes down.
Q: Why can’t people who suspect they have celiac just stop eating gluten?
A: It’s important to get tested before you self-prescribe a gluten-free diet. Once the diet begins, the clock starts ticking. The antibody blood tests and biopsy findings become normal over time once you remove gluten from the diet. So your tests could come back negative even if you have celiac disease.
Q: But if you’ve stopped eating gluten, why should that matter?
A: Celiac disease increases the risk of other health issues like infertility, cancer, osteoporosis, and other autoimmune diseases, so it’s important for you and your doctor to know. And since celiac runs in families, you can alert family members to get tested.
Q: What’s the difference between celiac disease and gluten sensitivity?
A: Non-celiac gluten sensitivity is poorly understood. The symptoms—which can mimic those of celiac—seem to be triggered by gluten or wheat, but there are no blood markers or intestinal damage like you see in celiac disease. We don’t have a reliable biomarker to identify gluten sensitivity. It’s based on an individual’s experience and history, assuming celiac disease has been thoroughly ruled out.
Bye bye gluten
Q: How is celiac disease managed?
A: The most important thing is to see a dietitian who’s an expert in a gluten-free diet. There’s a lot of information online, but it’s often mixed with misinformation. And, especially in social media groups, it is very common to see one-upsmanship in terms of the vigilance that’s required to avoid gluten.
Q: Is a gluten-free diet hard to stick to?
A: Most people with celiac disease do very well, their symptoms resolve, and their intestines heal. But nearly everyone gets inadvertently exposed to gluten at some point. If it’s occasional enough, it doesn’t cause any substantial clinical consequences. But some people have ongoing symptoms despite trying to be gluten-free, which could be due to inadvertent gluten exposure.
Q: How does gluten slip in to people’s diets?
A: “Gluten-free” labels on packaged foods can be trusted. But restaurants may be another story. We did an analysis of a crowdsourced opt-in app that was used by owners of a portable gluten sensor who tested various restaurant foods. Gluten was detected in about a third of all the foods—and in about half of the pastas and pizzas—that were labeled “gluten-free."
This was all voluntary reporting, so users may have only entered data when it was perhaps a bit more surprising or interesting. Still, we do believe there is a problem with restaurant foods.
Q: Why do pasta and pizza seem to be more of a problem?
A: Gluten-free pasta might be prepared in a pot of water that recently had regular pasta. Or gluten-free pizza might share oven space with gluten-containing pizza.
Q: Is there any reason to avoid gluten if you aren’t sensitive to it?
A: There are claims that a gluten-free diet offers benefits for cardiovascular health, cancer risk, blood sugar, cognition, and more, but there’s really no evidence to support that. And the gluten-free diet is often higher in sugar and fat and lower in fiber. So why try it if you don’t need to?
Q: Can pills that digest gluten protect against inadvertent gluten exposure?
A: There are two categories of gluten-digestive agents. One kind is being developed under rigorous clinical testing through an FDA-approval pathway. And it is showing promise in early clinical testing.
Unfortunately, the larger category—and what’s available to consumers now—is over-the-counter supplements. The few studies that have evaluated them have shown that they do not break down gluten sufficiently to be useful for people with celiac disease.
Q: What’s in the pipeline?
A: A growing number of non-dietary therapies are being tested. Some are drugs that would make the immune system more tolerant of gluten. The drugs, which are in various phases of clinical testing, would afford additional protection when inevitable gluten exposure occurs. Others may allow people to eventually eat a gluten-containing diet, though that’s a distant goal.
How to eat gluten-free
A gluten-free diet can be as healthy, delicious, and adventurous as any other.
Fruits, vegetables, beans, dairy, nuts, meat, poultry, and seafood are naturally gluten-free, says Anne Lee, assistant professor of nutritional medicine at the Celiac Disease Center at Columbia University. Only wheat, barley, and rye—or foods contaminated with those grains—are off the table.

Here are Lee’s other tips:
- “Gluten-free” labels. If a packaged food says it’s “gluten-free,” you can generally trust it. But it’s always a good idea—especially for traditionally flour-based foods like pasta, bread, cereal, crackers, and baked goods—to also check the ingredients for wheat, barley, rye, or malt (which is made from barley). Other no-noes: soy sauce and brewer’s yeast (unless they’re labeled “gluten-free").
- Gluten-free... and junkier. Many gluten-free breads, crackers, cookies, etc., add starches from potato, rice, corn, or tapioca, so they fall short on fiber. And plenty try to improve their texture and flavor by bumping up the sugar, salt, or fat.
- Good grains. Whole grains like quinoa, brown rice, millet, amaranth, sorghum, and buckwheat are safe.
- Alcohol. You can’t trust that all the gluten has been taken out of “gluten-removed” beer. Skip it. Wine is safe, as are all distilled spirits (including rye whiskey).
Want more info? Check out celiac.org/gluten-free-living/gluten-free-foods.
4 gluten-free supermarket finds
Editor's Note: This article comes from Nutrition Action. We don't accept any paid advertising or corporate or government donations. Any products we recommend have been vetted by our staff and are not advertisements by the manufacturers.

Oats are naturally gluten-free, but they can be contaminated with gluten if they’ve been grown in the same fields—or processed on the same equipment—as wheat, barley, or rye.
So if you’re avoiding gluten, look for oats labeled or certified “gluten-free.” Baking? Try gluten-free oat flour. Or toss gluten-free rolled oats into a food processor or blender to grind your own.

Whole-grain, organic Mary’s Gone Crackers are mostly brown rice, quinoa, flax seeds, and sesame seeds, with no added starches. That adds up to a nice 3 grams of fiber per 12-cracker serving...and a whole lot of crunch. Mary’s Super Seed crackers have the same main ingredients, plus pumpkin and sunflower seeds.

Gluten-free pasta with as much fiber as whole-wheat pasta—and more protein? Yup.
Say hello to legume pastas. Brands like Barilla and Tolerant Organic have just one ingredient: lentil (or chickpea) flour.
Tip: They cook quickly. To avoid gummy pasta, check the cook time before you turn on the burner.

Most gluten-free breads have added starches (see “How to eat gluten-free” above).
But Outer Aisle Original Cauliflower Sandwich Thins skip the grains altogether. Instead, there’s real cauliflower plus a little egg, parmesan, and nutritional yeast. Lightly toast them under the broiler. Mmm.
Continue reading this article with a NutritionAction subscription
Already a subscriber? Log in

Let's stay in touch
Get our (free) healthy tips
Our free Healthy Tips newsletter offers a peek at what Nutrition Action subscribers get—scrupulously researched advice about food of all kinds, staying healthy with diet and exercise, and more.