
Asier - stock.adobe.com.
This article is free for a limited time. Subscribe to access every article and recipe.
More than half of middle-aged and older adults have lower urinary tract symptoms (LUTS). That can include urinary leakage, urgency, and frequent visits to the bathroom, day or night. Others experience recurrent urinary tract infections or painful kidney stones.
Here’s what to know about keeping your urinary tract in shape.
1. LUTS aren’t rare.
LUTS are a common but often well-kept secret.
“Most patients first suffer through the embarrassment and have no one to discuss it with,” explained retired interior designer Lynn Kiley, describing her experience with incontinence at a webinar hosted by the Agency for Healthcare Research and Quality in October.
“Until my 39-year-old niece introduced me to urogynecology, I did not receive any treatment for 25 years, although I sought it.”
Common LUTS symptoms
LUTS don’t always include incontinence. The key symptoms: “Urinary urgency, frequency, and having to urinate at night,” says Alayne Markland, professor of medicine at the University of Alabama at Birmingham and researcher at the Birmingham VA Health Care System.
Those symptoms—with or without incontinence—are often grouped together as “overactive bladder.”
“LUTS can also include problems like post-void dribbling, incomplete emptying of the bladder, or stopping and starting urine flow,” notes Markland.
And LUTS are more common than people think.
“In most population-based studies, 60 to 70 percent of women have urinary symptoms,” says Markland. The percentage in men is similar.
What typically causes LUTS?
“In women, childbirth, hormonal changes, and menopause can increase the risk,” says Markland.
“Pregnancy and a vaginal delivery stretch the pelvic floor,” she explains. Injuries caused by forceps or prolonged labor may cause further damage.
The pelvic floor is the ring of muscles that sit under the bladder.
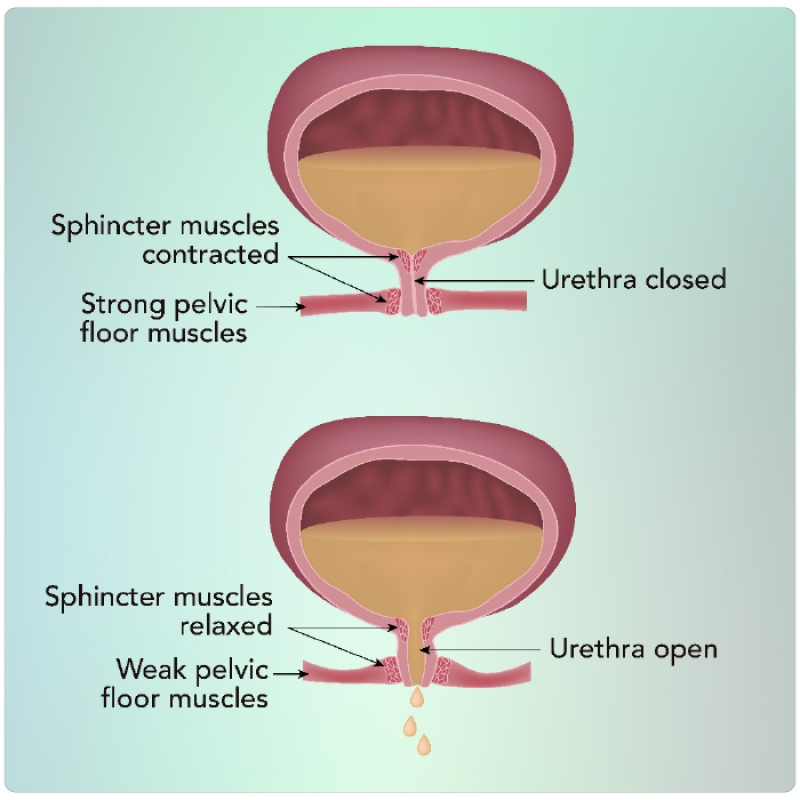
“In both men and women, pelvic floor muscles make up the sphincter around the urethra that gives us the ability to hold urine until we get to the bathroom,” says Markland.
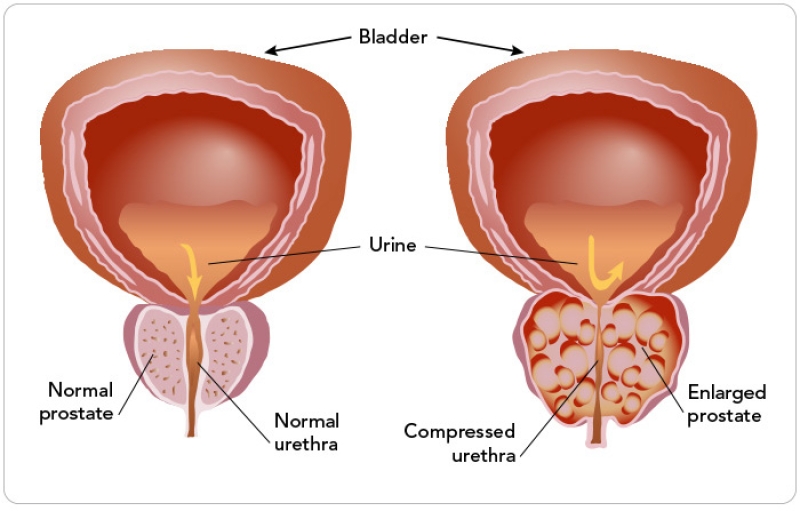
“In men, urinary symptoms are usually related to an enlarged prostate, prostate cancer, or prostate cancer treatment.”
Since the prostate wraps around the urethra (see "Benign prostatic hyperplasia”), an enlarged prostate—either benign or due to cancer—can block urine flow. And surgery or radiation to treat prostate cancer can damage nerves, sphincters, or other tissues.
Two other risk factors for LUTS in both men and women: obesity and diabetes.
“Increased adiposity in the abdominal section can put pressure on the pelvic floor,” explains Markland. “And diabetes can cause nerve damage.”
Medications that can lead to LUTS
“The diuretics that many people need for blood pressure or heart problems are one of the worst, because they make you urinate a lot more,” says Markland.
Antidepressants, antihistamines, bronchodilators, and sedatives are among the other drugs that can cause LUTS.
“And some opioids, narcotics, or medicines for neuropathy can dull the sensation of bladder fullness,” adds Markland.
Got symptoms? Check the package insert of any drugs you take.
More importantly, check with your doctor to find out what’s causing your symptoms. They may be due to a neurological disease, cancer, or other illness.
2. LUTS can be treated.
A major misconception about LUTS: “People think it’s just a normal part of aging and there’s nothing you can do about it,” says Markland.
“There’s a lot of marketing for absorptive pads and underwear, and they do make people feel confident and improve their ability to be active. But people should try to treat the problem rather than just contain it.” What works?
Pelvic floor muscle training
These exercises repeatedly tighten, hold, and relax pelvic floor muscles.
“We found that women who did pelvic floor muscle training supervised by a physical therapist were eight times more likely to report being cured of stress incontinence than those who did no training,” says professor Chantale Dumoulin of the faculty of medicine at the Université de Montréal.”
“Stress urinary incontinence happens when you cough or sneeze,” explains Dumoulin, who is also the Canadian Research Chair in Urogynecological Health and Aging.
“Training was a bit less effective for urgency incontinence, which occurs when you have an urgent need to go to the bathroom.”
That’s probably because urgency is more complicated, she adds. “It occurs not only because the pelvic muscle is weak, but because the bladder is hyperactive.”
Dumoulin randomly assigned 319 women aged 60 or older who had incontinence to do 12 weeks of pelvic floor training either individually or in groups of eight supervised by a physical therapist. Both had weekly one-hour sessions including 45 minutes of exercises that were increasingly difficult over time, plus home exercises 3 to 5 days a week.
The results: “A year after the training sessions began, incontinence episodes had dropped by 70 percent in the individuals and by 74 percent in the groups,” says Dumoulin. “So both were effective.”
And group training had a bonus. “The women felt part of a community,” says Dumoulin. “Incontinence is stigmatizing. But these women felt empowered. They were taking charge of their health, and they were doing it together.”
Ultrasound images confirmed that training had changed the women’s pelvic floor muscles.
“A year after the training, the muscle was more tight, showing that it had improved function,” explains Dumoulin.
“It’s never too late to train. We can see changes in muscle and in symptoms even if you’re 60, 70, or 80 years old.”
And pelvic floor muscle training isn’t just for women...or just for incontinence.
Behavioral changes
The University of Alabama at Birmingham’s Alayne Markland and colleagues randomly assigned 204 men with overactive bladder to six weeks of behavioral therapy, drug therapy, or both. The drugs were an antimuscarinic (tolterodine) plus an alpha blocker (tamsulosin). The behavior therapy included:
- pelvic floor muscle exercise,
- restricting fluids 3 hours before bed,
- delayed voiding, and
- urge suppression strategies.
One technique to suppress the urge to urinate: “You can contract your pelvic floor muscles eight times,” says Dumoulin. “That will send a message to the bladder to calm down.”
The results: Behavioral therapy—with or without the drugs—curbed urinary frequency better than the drugs alone, which aren’t terribly effective.
“I often take a first-line approach that starts with behavior, not medicine,” says Markland.
Liquids
Cutting back on liquids may help with LUTS. “There are lots of apps and products suggesting that people should drink outrageous amounts of fluid,” says Megan Schimpf, professor of obstetrics and gynecology and urology at the University of Michigan.
“I see women with huge jugs of water that they feel compelled to drink by the end of the day. Well, if you’re drinking five liters of water a day, you’re going to urinate a good portion of that out.”
Caffeine is a diuretic, so cutting back may help. But the few clinical trials that tested its impact on bladder symptoms were small and shaky.
So Schimpf and her colleagues randomly assigned 105 women with overactive bladder either to replace “potentially irritating” beverages with water or milk or to a control group that got advice about healthy eating.
“Potentially irritating” was anything caffeinated, alcoholic, carbonated, artificially sweetened, or acidic.
But after two weeks, there was no difference in urinary frequency or urgency.
It’s not clear why. One possibility: “We didn’t succeed very well at getting people to trade coffee for milk and water,” notes Schimpf. Or “potentially irritating” beverages may not matter.
Bottom line: If you have an overactive bladder, try cutting back on caffeine to see if it helps.
3. Men have new options to treat benign prostatic hyperplasia.
In men, benign prostatic hyperplasia (BPH)—often called an enlarged prostate—is the major cause of LUTS.
Most men with BPH are treated with drugs like the phosphodiesterase-5 inhibitor tadalafil (Cialis), alpha blockers like tamsulosin (Flomax), and/or 5-alpha reductase inhibitors (5-ARIs) like finasteride (Proscar).
But the alpha blockers can cause side effects like lightheadedness, ejaculatory dysfunction, and headaches. And the 5-ARIs can cause erectile dysfunction, decreased libido, enlarged breasts, and an increased risk of aggressive prostate cancer.
“I covered the Detroit VA for a number of years recently, and at the time when VAs had 500, 600-patient waiting lists for clinic, we were seeing patients on triple drug therapy who still had high [symptom] scores,” said Michael Harris, a urologist now at the Novello Specialty Clinic in Traverse City, Michigan, at the 2nd Annual Advances in Men’s Health Conference in August.
“And I was told, ‘Well, we don’t have time to TURP all these guys,’” recalled Harris, referring to a transurethral resection of the prostate, which trims away excess prostate tissue that’s blocking urine flow.
And over time, the drugs had a downside. “We saw a lot of decompensated bladders,” said Harris. In other words, the bladder was losing its ability to function properly.
New minimally invasive surgeries to treat BPH
From the 1960s to the 1980s, a TURP “was the number-one treatment for BPH,” noted Harris. “It was the gold standard.”
These days, urologists are switching to minimally invasive surgical therapies (MISTs).
Among the most popular: UroLift, which “uses small implants to hold open the obstructed pathway that’s blocking urine flow,” and Rezūm, which uses water vapor to “remove excess prostate tissue that is pressing on the urethra,” according to the companies.
“The MISTs have advantages,” explained Harris. “You can do most of these things in the office. It’s an anatomic treatment so you’re addressing the obstruction, [patients have a] quick recovery, [it’s] less expensive than a hospital stay, and [there’s] minimal sexual impact. You don’t get retrograde ejaculation like you will with a well-done TURP. And if you still have troubles, you can come back and do a TURP later.”
The results are less dramatic than with a TURP, he acknowledged. “But when you look at the satisfaction scores, they’re fairly close.”
That said, long-term randomized trials are lacking.
The evidence for UroLift and Rezūm
In industry-funded studies on both UroLift and Rezūm, men who were randomly assigned to those procedures had significantly fewer symptoms than those assigned to a “sham” treatment.
But those trials only lasted for three months, after which men in the “sham” groups were offered the real thing.
However, noted Harris, “with UroLift you’ve got real-world database experience [on] over 3,000 cases...and with Rezūm, over 250.” His take: “This is an anatomic problem, so we really have to address the anatomy, whereas the medical therapy is addressing symptoms."
4. UTI advice is often iffy.
“When I was training to be a urologist in the late ‘90s and early 2000s, we used to give out Cipro like candy over the phone when women had symptoms of a UTI,” says Jennifer Anger, professor of urology at the University of California San Diego.
(She’s referring to ciprofloxacin, an antibiotic that’s used to treat a broad spectrum of bacteria.)
But that led to collateral damage. “A large proportion of patients developed urinary tract infections with bacteria that were resistant to many antibiotics,” explains Anger, who led a recent review of the American Urological Association's guidelines for treating recurrent UTIs.
What’s more, antibiotics can cause side effects. “For example, fluoroquinolones are associated with muscle soreness, and even Achilles tendon ruptures,” notes Anger.
Antibiotics can also lead to dysbiosis. “That’s where we lose the healthy, protective flora of the GI tract and vagina,” says Anger. “So women may develop serious Clostridium difficile infections in the GI tract or bacterial vaginosis or yeast infections.”
Today, Anger sends a urine sample to a lab to see which bacteria it contains. Then she prescribes an antibiotic that targets that patient’s bacteria.
“We also take into account the local antibiogram, which tells us the antibiotic resistance patterns in our geographic location,” she adds.
What hasn’t changed—iffy evidence about preventing UTIs.
Anger and her colleagues examined social media posts to see what people were recommending for UTIs in women. Nearly half of the advice—like avoiding alcohol, caffeine, citrus, or sugar—was backed by little or no evidence.
“People swear by something, and that causes increased use,” she says. “That may not cause any harm, but we don’t have enough evidence that it works.”
Here’s the scoop on some other strategies for preventing UTIs:
Fluids
Scientists randomly assigned 140 premenopausal women with recurrent UTIs who typically drank less than 1½ liters—a little over six cups—of fluids a day to drink either an extra 1½ liters of water or no extra water.
Over the next 12 months, the extra-water drinkers averaged 1.7 UTIs versus 3.2 in the no-extra-water group. (Some of the scientists were from Danone Research. Danone sells bottled water.)
“It’s just one study, but other than that, there’s not much evidence on diet,” says Anger.
Vaginal estrogen
“After menopause, the vagina becomes less acidic,” explains Anger. “Vaginal estrogen may restore a healthy acidic pH.” That may explain why it lowered the risk of UTIs in five studies.
And, unlike the estrogen that’s swallowed, estrogen inserted into the vagina doesn’t raise levels of estrogen in the blood. “There’s no evidence that it causes cancer, even in women with a history of breast cancer,” says Anger.
Cranberry
In 2020, the FDA found only “limited” evidence that cranberry supplements could prevent UTIs. The evidence for cranberry beverages was “limited and inconsistent.”
What’s more, downing a daily cup of cranberry juice cocktail in hopes of preventing a future UTI adds 5½ teaspoons of added sugar—half a day’s worth—to your diet day after day.
D-mannose
D-mannose is a sugar found in fruits like grapes and apples. In test tubes, it seems to keep E. coli bacteria from binding to urinary tract cells. But a rigorous 2022 review of human studies concluded that “there is not enough evidence to know whether D-mannose prevents or treats acute or recurrent UTIs.”
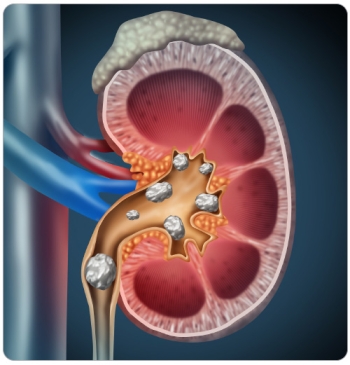
5. You may be confused about kidney stones.
Most people don’t think about kidney stones until they’ve had one. But here’s what may affect your risk of that first—or subsequent—stone.
Oxalate
Spinach is high in oxalate, which can promote calcium oxalate kidney stones, the most common type.
“But I just had a call with a patient who said, ‘I guess I can’t eat kale,’” says Gary Curhan, a nephrologist at Brigham and Women’s Hospital and professor of epidemiology at the Harvard T.H. Chan School of Public Health.
“Well, kale is not high in oxalate. You don’t have to avoid all green leafy vegetables if you’ve had a kidney stone.”
Likewise, you needn’t avoid all nuts. “The range of oxalate in nuts varies,” says Curhan. “Pistachios are one of the lowest. Almonds are the highest.”
Beets are also high in oxalate. “Potatoes aren’t as high,” he adds, “but people eat a lot so they should also be avoided.”
Lemon
“Citrate is a natural inhibitor of kidney stone formation, so people think, ‘If I put lemon in my water that helps,’” says Curhan. “But a spray of lemon doesn’t get your urine citrate up.”
Liquids
Getting enough fluids may curb your risk by diluting your urine. And water isn’t your only option.
Coffee
Coffee drinkers consistently have a lower risk of getting a first kidney stone. “We initially thought it was just caffeine, because it increases urine output,” says Curhan. “But decaf drinkers also have a lower risk.”
Tea
“Some people don’t drink tea because they’ve heard that it’s very high in oxalate,” says Curhan. But each cup has just 15 milligrams, far less than spinach (655 mg per cup if raw). “And tea drinkers have a lower risk of getting a first stone,” he adds.
Alcohol
Does alcohol cause kidney stones because it’s dehydrating? “I’m not encouraging people to drink alcohol, but the idea that you can’t have any is just incorrect,” notes Curhan. In contrast, sugary drinks are linked to a higher risk.
Calcium
Women who were randomly assigned to take 1,000 mg of calcium a day (in addition to the roughly 1,150 mg they were getting from their own supplements and diet) for seven years had a 17 percent higher risk of kidney stones than those who got 1,150 mg from their diet and supplements and took a placebo. But calcium in foods may lower risk.
“When you eat food, calcium and oxalate form a crystal in the intestine and are excreted in the stool,” explains Curhan. “That keeps the oxalate from getting absorbed into the blood and eventually reaching the urine, where it—and any excess calcium—can form kidney stones.”
If you need a calcium supplement, take it with meals, he advises.
Sodium
“A higher sodium intake increases calcium excretion,” says Curhan. “That’s one more reason to eat a lower-sodium diet.”
A Mediterranean or DASH diet
Both are linked to a lower risk of stones. It’s not clear why. “Diets that are rich in fruits and vegetables will raise your citrate, a natural inhibitor of stone formation,” says Curhan. “And vegetables contain more water than many other foods.”
His advice: “I can’t be sure that those diets will cut your risk of stones, but they will reduce your risk of cardiovascular disease.”
Want to protect your heart, eat plenty of fruits and veggies, and more?
A healthy DASH-style way of eating may cut your risk of kidney stones. And it also lowers your risk of cardiovascular disease. So why not give it a try?
The latest on preventing disease
What’s behind the Viagra and Alzheimer’s study?

Can a healthy diet lower the risk of breast cancer recurring?

What to know about 4 common toxic elements

A vaccine that prevents cervical cancer

Is there a risk of cancer from ultra-processed foods?
